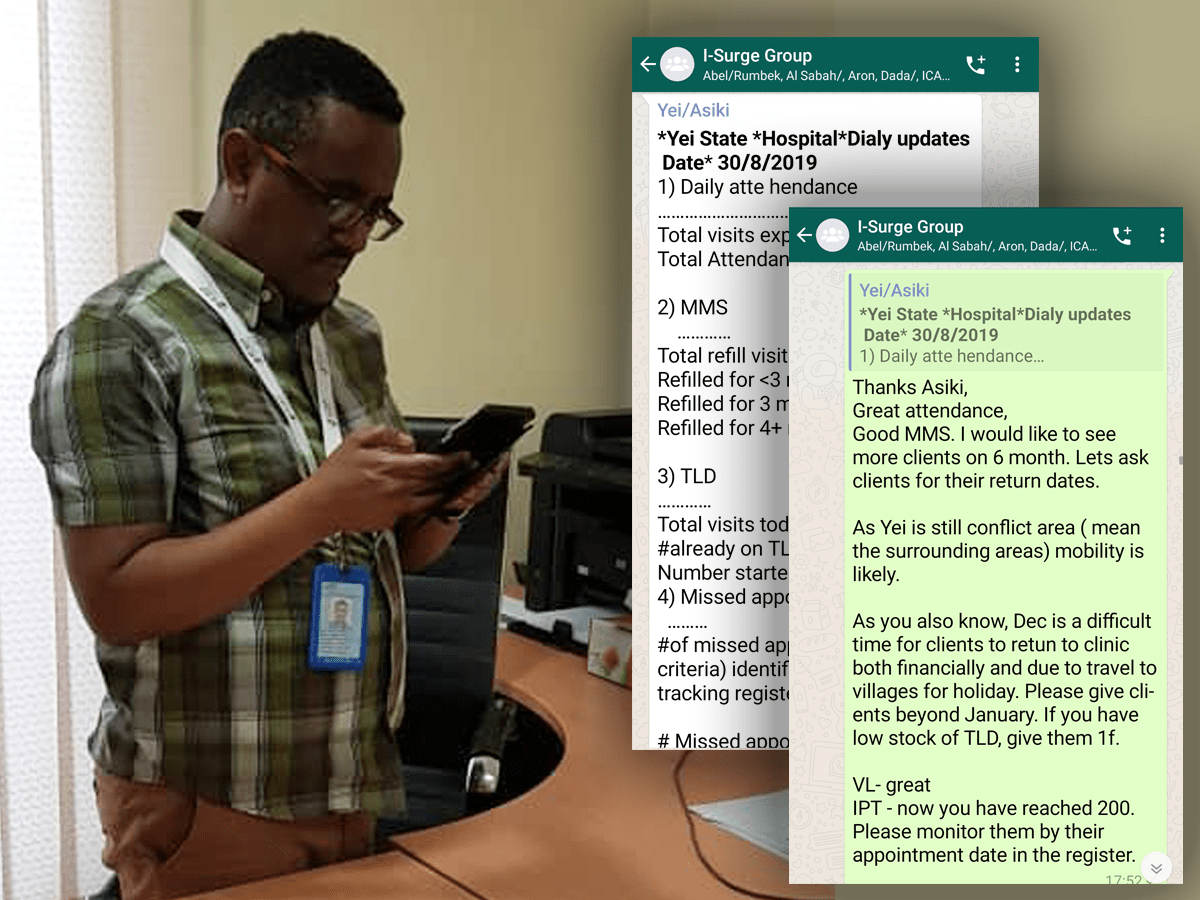
At ICAP’s office in Juba, South Sudan, Shambel Aragaw’s phone buzzes. Aragaw, a medical doctor, is the technical director for ICAP in South Sudan, and the buzz is a WhatsApp notification. But not just any notification. This is the daily summary of all HIV-related activities at one of the 14 sites ICAP supports across the country.
“The WhatsApp group includes all the facility-based points-of-contact and data clerks, as well as the ICAP team here in the office,” Aragaw said. “Every day, we get a report from the point-of-contact at each facility covering the entire HIV cascade, from testing to treatment to viral load monitoring, and then we provide same-day feedback about data quality, gaps, and possible resolutions. This fast turnaround helps to improve processes and outcomes in real time, and because everyone is on the thread, there are opportunities to see how other sites are performing and either borrow ideas or offer support.”
The WhatsApp group is just one part of ICAP’s “I-Surge” approach, which uses intensive site support, daily monitoring and reporting, and fast turnaround of feedback to drive rapid improvements along the HIV cascade. With support from the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC), ICAP is implementing this approach in high- and medium-HIV priority locations in eight of South Sudan’s 32 states.
What makes the I-Surge strategy such a gamechanger is ICAP’s model of site-level support and daily data management. In order to make annual performance targets more manageable, ICAP assisted the designated point-of-contact at each facility to break down the yearly goal into monthly, weekly, and daily targets. ICAP also developed a standardized, simplified reporting format for all key indicators, so each testing and treatment unit at every health facility is using the same template, and the results are easy to review, summarize, and roll up into weekly and monthly reports.
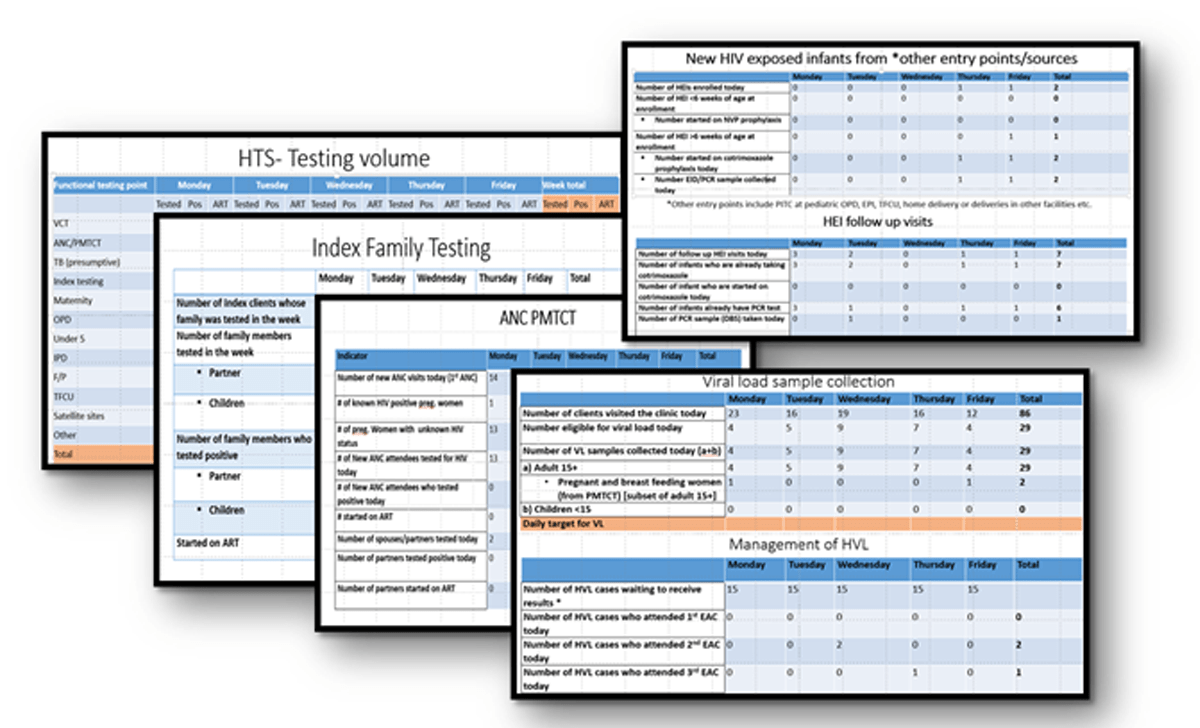
Every day, following consultation with their counterpart in the ICAP office in Juba, each point-of-contact sends their facility’s report to the WhatsApp group for same-day feedback. This helps to identify site-specific gaps, which they can communicate back to the testing and treatment teams along with any adjustments to the assigned daily targets.
“The WhatsApp group is also a place to share experiences and challenges,” said Isaac Avaku, the point-of-contact at Juba Teaching hospital. “It provides an opportunity for quick intervention, in case something is urgent, and it’s great to see what everyone else submits so we can learn from one another and get a sense of the big picture!”
Thanks to these combined efforts, the number of people who tested positive for HIV (a measure of effective case finding, for example via index testing) rose by 44 percent over the course of a single year, and the number of people diagnosed with HIV being linked to care increased by 84 percent, helping to close the gap and move toward a 100 percent linkage-to-care rate.
“We have also started tracking and forecasting patient flow based on the number of people we expect at the clinic versus the number who came either with or without an appointment,” said Avaku. “This helps with scheduling, so we aren’t overstaffed or understaffed, and it also helps us set targets for our key performance indicators if we know we will have a busy or a slow day.”
Based on the success of the I-Surge approach in improving case identification and linkage to care, ICAP in South Sudan has started to apply this model to other areas, including retention in care, data capture and management, clinical systems proficiency for HIV focal persons, due-date tracking for pregnant patients living with HIV, and tracing of clients who have missed appointments and are lost to follow-up.
“The I-Surge activities have set new heights for ICAP South Sudan, in terms of improving service delivery and achieving targets,” said Florence Bayoa, MA, country director for ICAP in South Sudan. “We believe that this approach will result in improved patient outcomes and program performance, which will help bring South Sudan closer to controlling the HIV epidemic.”
Additionally, this success has been noticed by CDC-South Sudan, which has commended the strategy as a model for other implementing partners to replicate. “ICAP’s I-Surge strategy is an excellent model that has put both PEPFAR and other treatment implementing partners on their toes,” said John Mondi, MBBS, MPH, prevention advisor for CDC-South Sudan. “It enables all of us to look at patients as individuals, not just numbers.”
A global health leader since 2003, ICAP was founded at Columbia University with one overarching goal: to improve the health of families and communities. Together with its partners—ministries of health, large multilaterals, health care providers, and patients—ICAP strives for a world where health is available to all. To date, ICAP has addressed major public health challenges and the needs of local health systems through 6,000 sites across more than 30 countries. For more information about ICAP, visit: icap.columbia.edu




